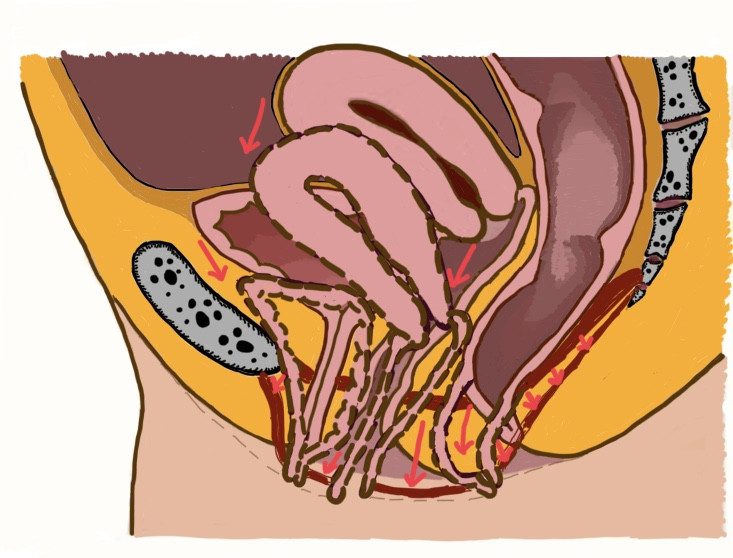
Pelvic floor descent is the relaxation/hanging of the pelvic floor. The pelvic floor is a muscle and connective tissue hammock supporting the pelvic organs. The hammock is attached to the internal frame of the pelvic bones. The pelvic organs – bladder, uterus, rectum in women and bladder, prostate and rectum in men are directly resting on this layer of muscles. Their exit tubes – the urethra, vagina and anal canal – cross the pelvic floor to open under it, on the perineum.
From chronic constipation, years of straining on the toilet, or from multiple pregnancies and difficult deliveries, the pelvic floor may become stretched, loose, hanging. This may affect the function of the organs supported by the pelvic floor: emptying of the bladder and rectum may become difficult or not possible fully. Or the opposite might happen: holding the urine or stool may become impaired. With the descent of the hammock organ prolapses i.e. bladder prolapse, uterine prolapse, rectal prolapse, rectocele or cystocele occur.
What signs and symptoms one has with these problems?
Pelvic floor descent can be mild, moderate or severe and can affect the front, middle or the back compartment of the pelvic floor or can affect the whole pelvic floor.
With mild pelvic floor descent the symptoms might be none or minimal, while with severe descent the symptoms are more marked.
Pain can be present or not, can be constant or only coming on exertion or after a long day. The pain, if present, is normally deep seated pelvi-perineal pain often radiating to the back.
With anterior pelvic floor descent the bladder will prolapse, this can cause urinary retention: difficulty or inability to completely empty the bladder. If the support of the neck of the urethra weakens, stress urinary incontinence occur: urine leaks a bit or more when coughing, jumping or sneezing. If the connective tissues in the front wall of the vagina weaken, the bladder can bulge towards the vagina: cystocele occurs.
The weakness of the middle compartment can cause uterine prolapse: the uterus falling downwards within the vagina.
When the back wall of the vagina weakens the rectum bulges into the vagina: rectocele occurs.
Cystocele, Uterine prolapse and Rectocele are all coming with the feeling of a lump inside the vagina and as they progress, the bulges may become visible outside.
With cystocele, other than the feeling of bulge in the vagina, most of the time difficulties with emptying the urine is present. It takes longer to pee, needs position changes to achive emptying and eventually retention occurs, i.e. the bladder will never fully empty, which can cause recurring urinary infections.
With rectocele, other than the feeling of bulge in the vagina, difficulties with emptying the stool can occur. After the bowel movement still something is felt inside the rectum, which is called incomplete evacuation. The emptying might be difficult. Many patient discovers simple manoeuvres to help emptying, like supporting the perineum or the posterior vaginal wall while straining.
Severe overall pelvic floor descent cause chronic pulling discomfort/pain, and a variety of the above symptoms from difficulties of emptying the rectum and or the bladder to reduced ability to control. Sensation deficits might be apparent. The patient is complaining of not feeling the urge to go to the toilet. Often a compensatory muscle tightening is present: trying to pull together the hanging hammock, which leads to anal pain and anal fissures.