- 99 patients with FI (Fecal Incontinence) with or without OD (Obstructed Defecation)
- Gender: 68 females, 21 males
- Age: 36 – 64; mean 47.2
- Home
- /
- For colleagues



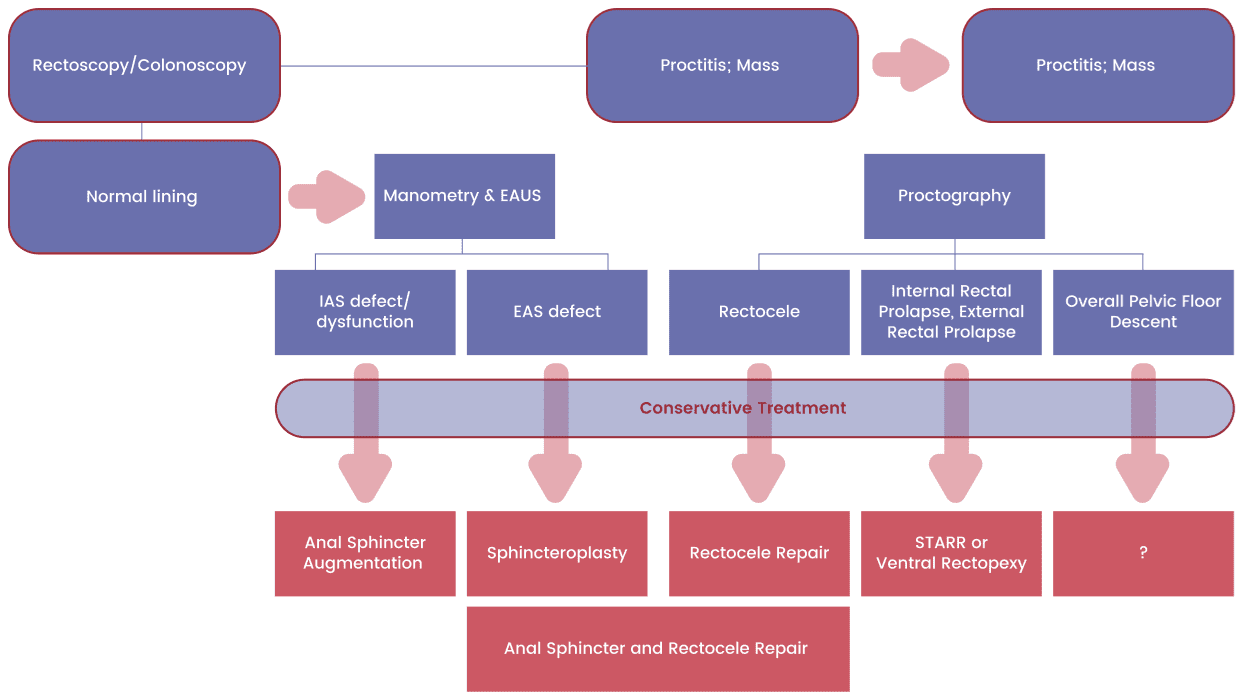
Conservative
Operative
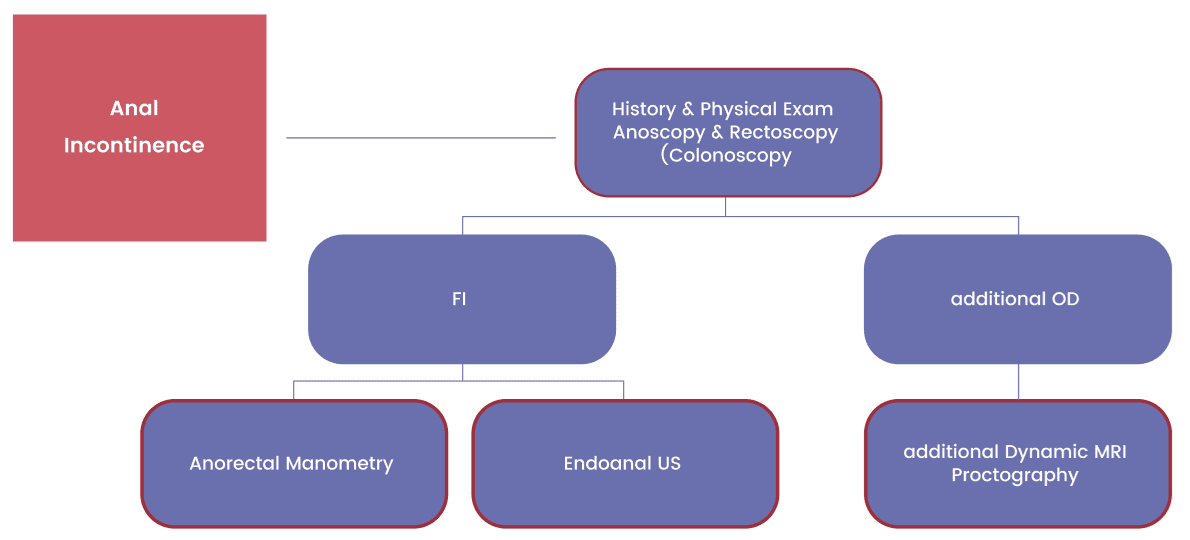
FI
FI & OD
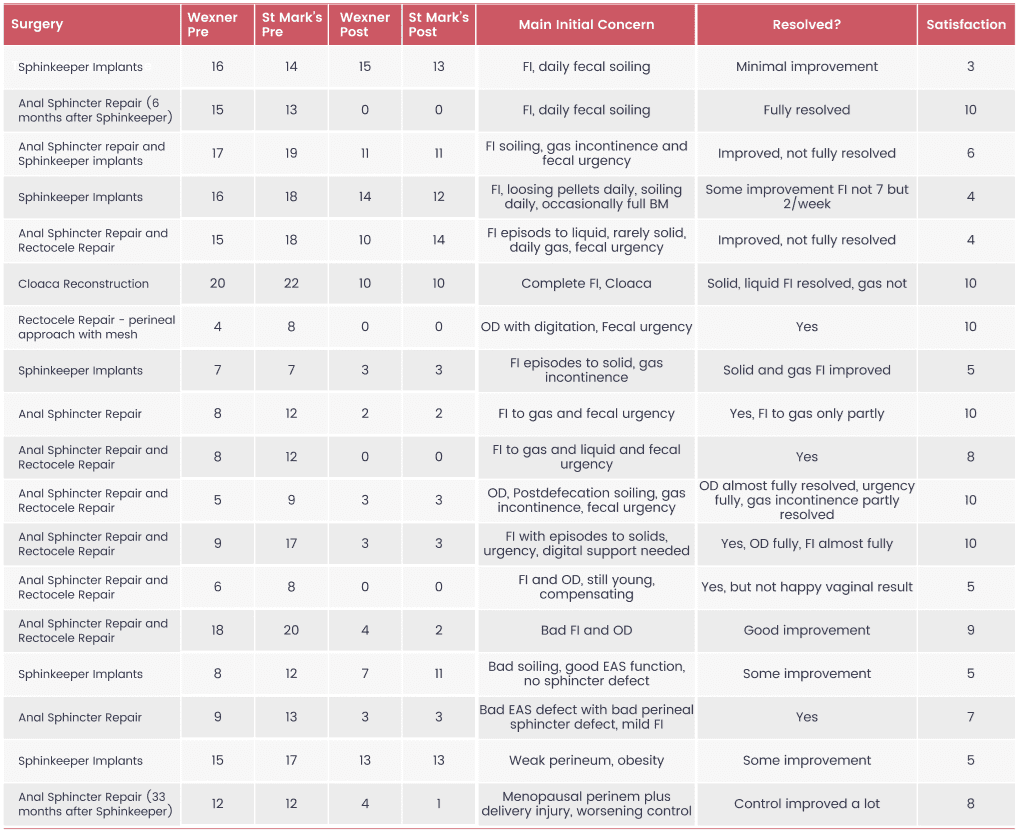
Of these 99 patient 19 had surgeries – 6 for both OD and FI; 5 for only FI and 3 for only OD
these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing

these photos contain sensitive content which some people may find offensive and disturbing

these photos contain sensitive content which some people may find offensive and disturbing

these photos contain sensitive content which some people may find offensive and disturbing

these photos contain sensitive content which some people may find offensive and disturbing

these photos contain sensitive content which some people may find offensive and disturbing

these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing

these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing

these photos contain sensitive content which some people may find offensive and disturbing

these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing

these photos contain sensitive content which some people may find offensive and disturbing

these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing

these photos contain sensitive content which some people may find offensive and disturbing
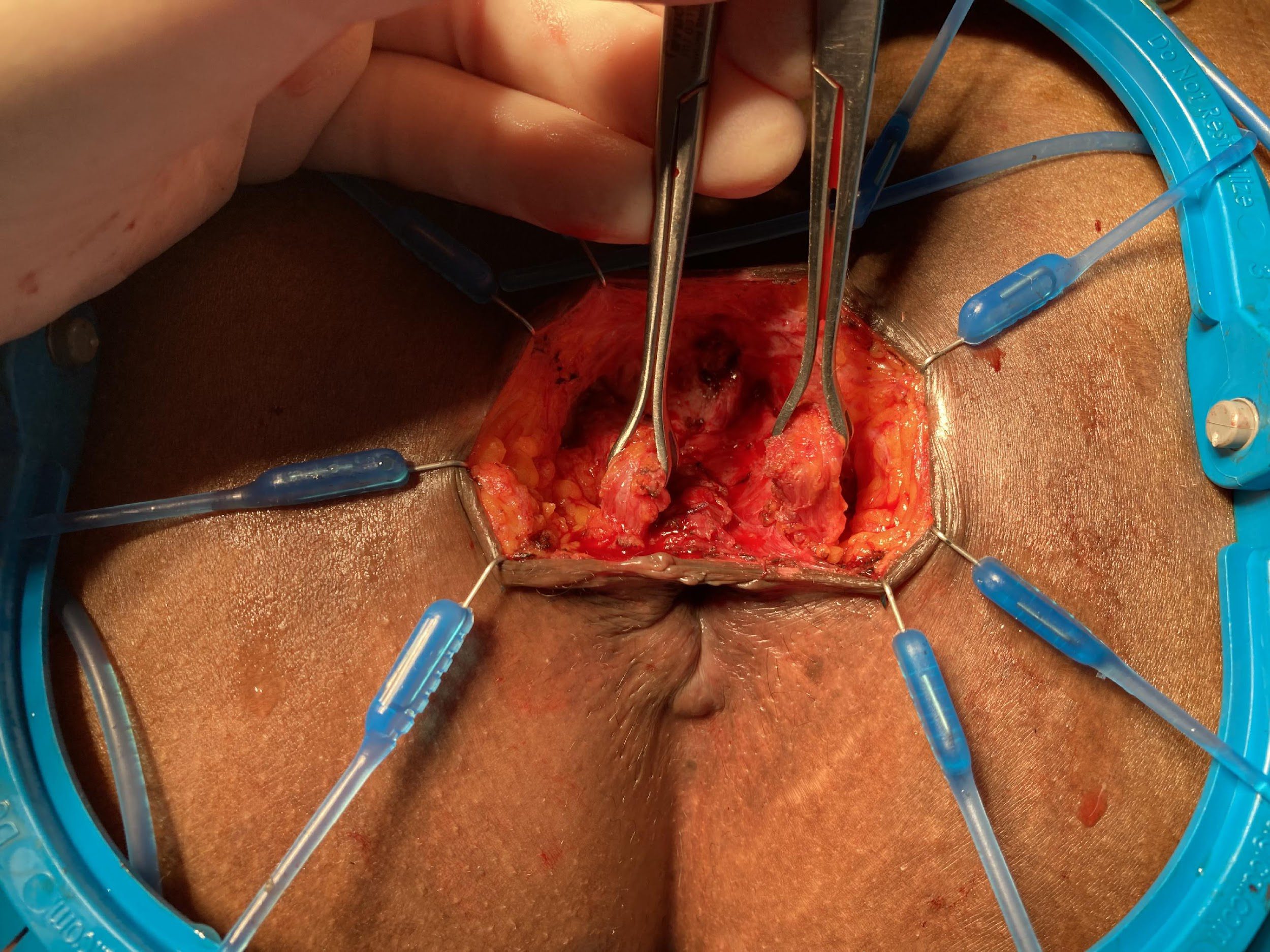
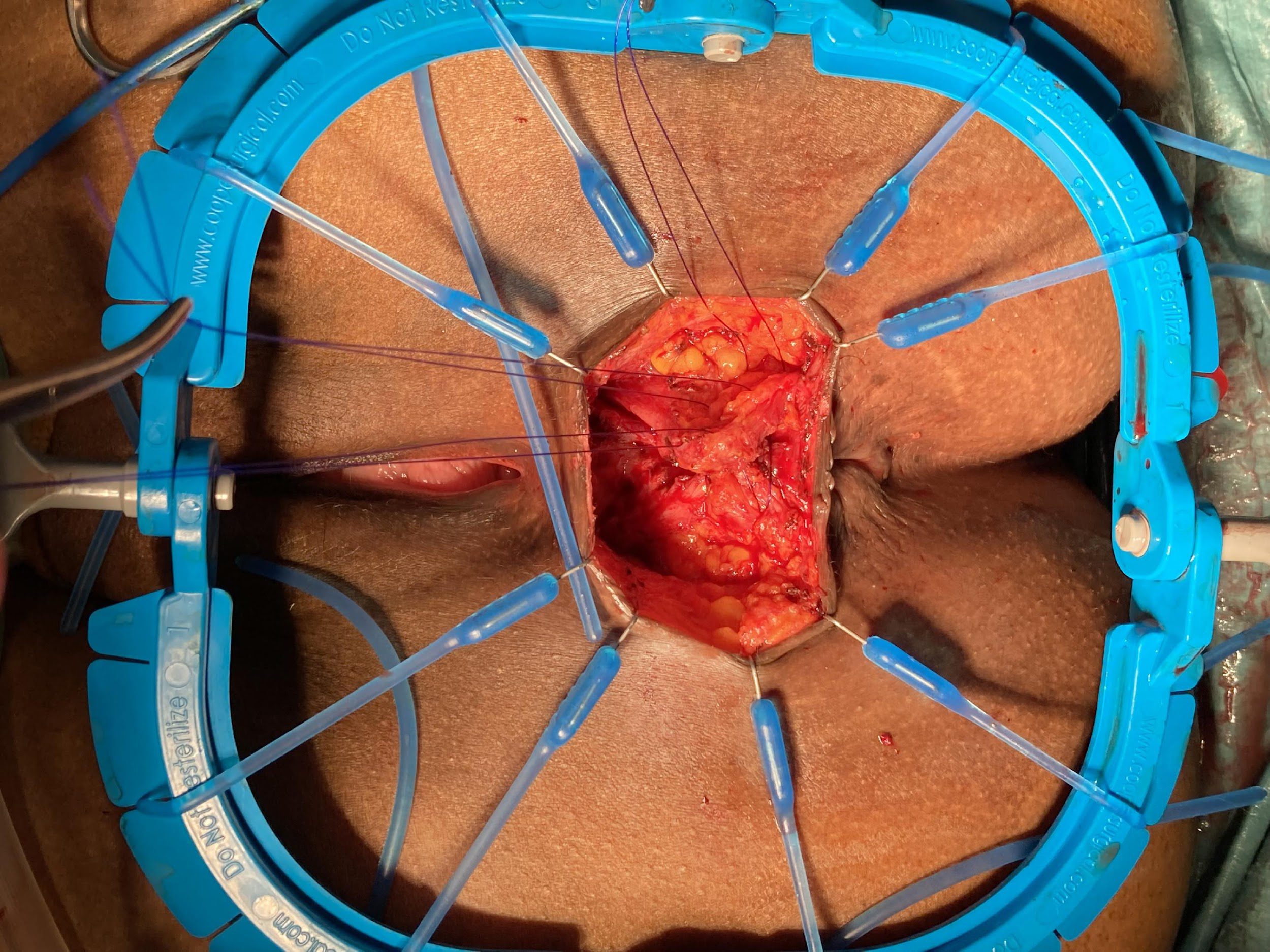
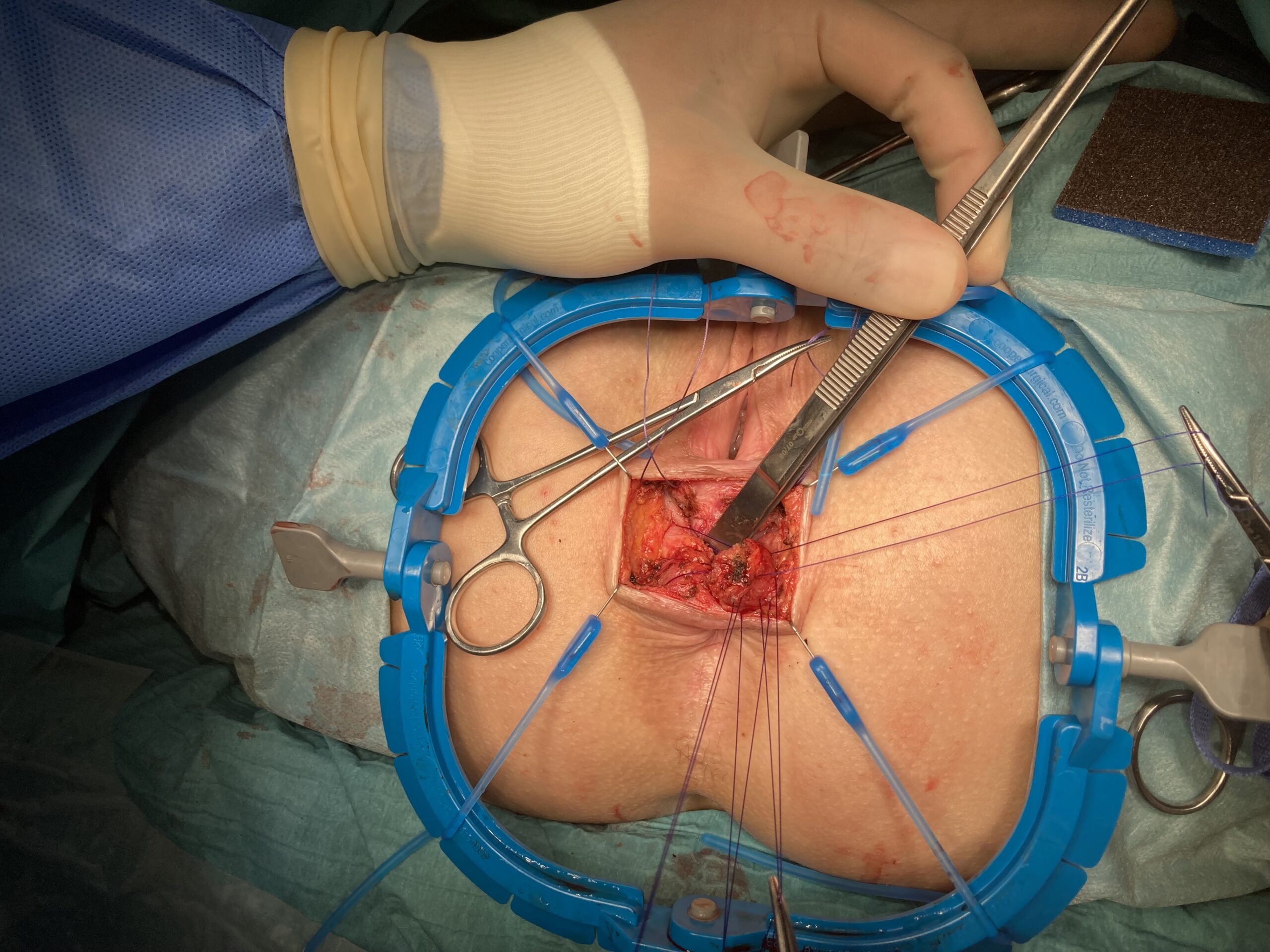
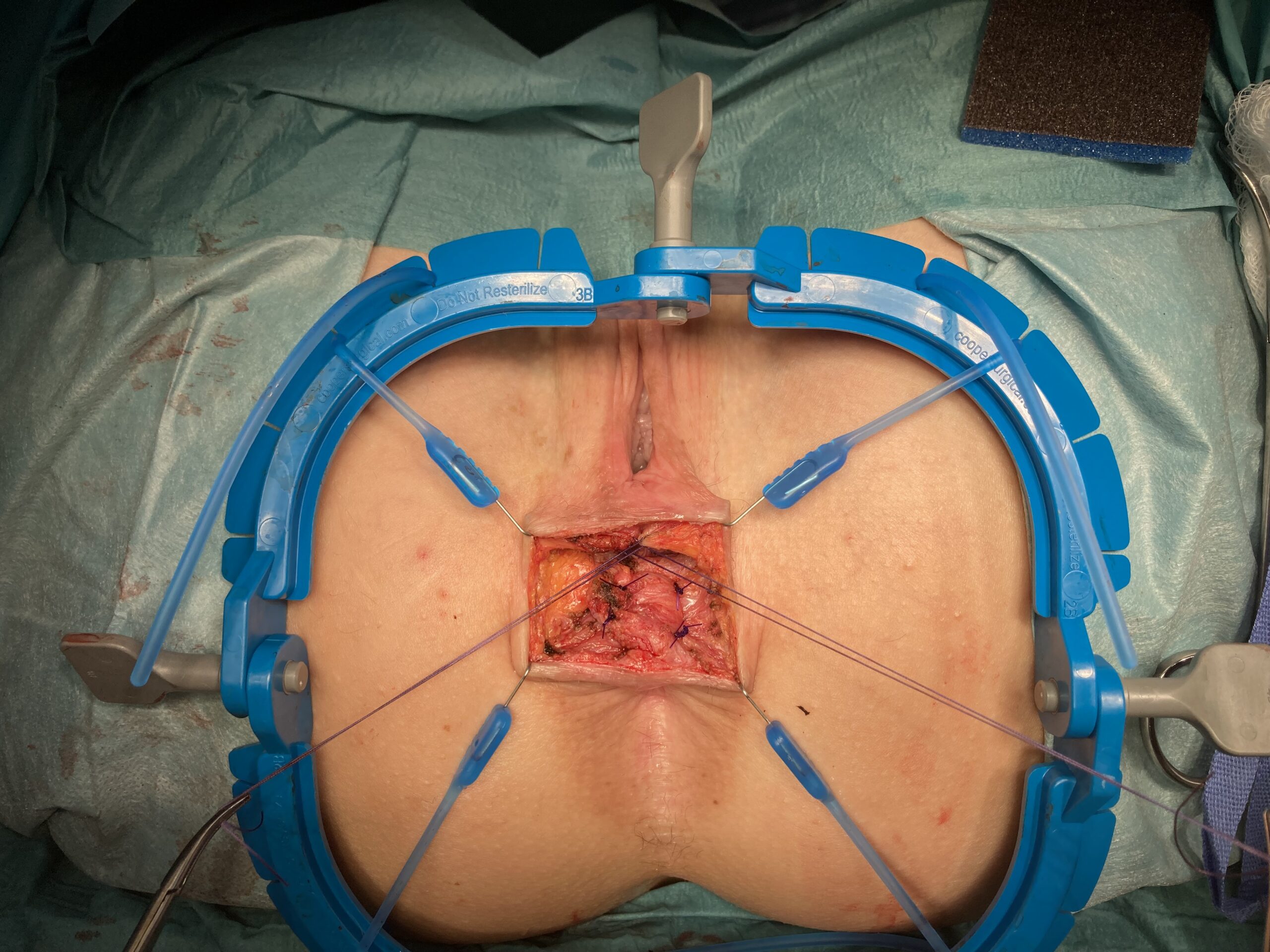
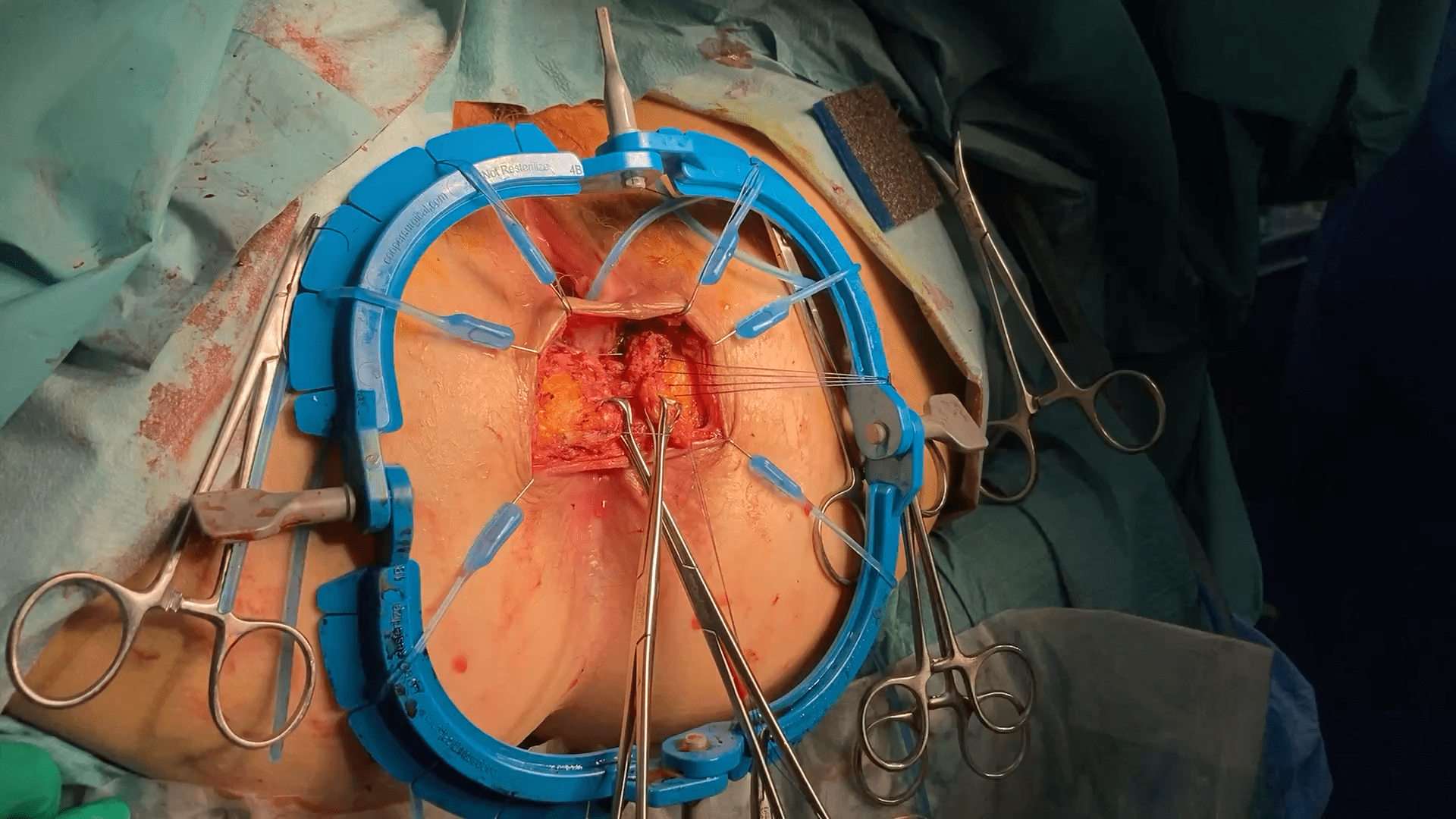
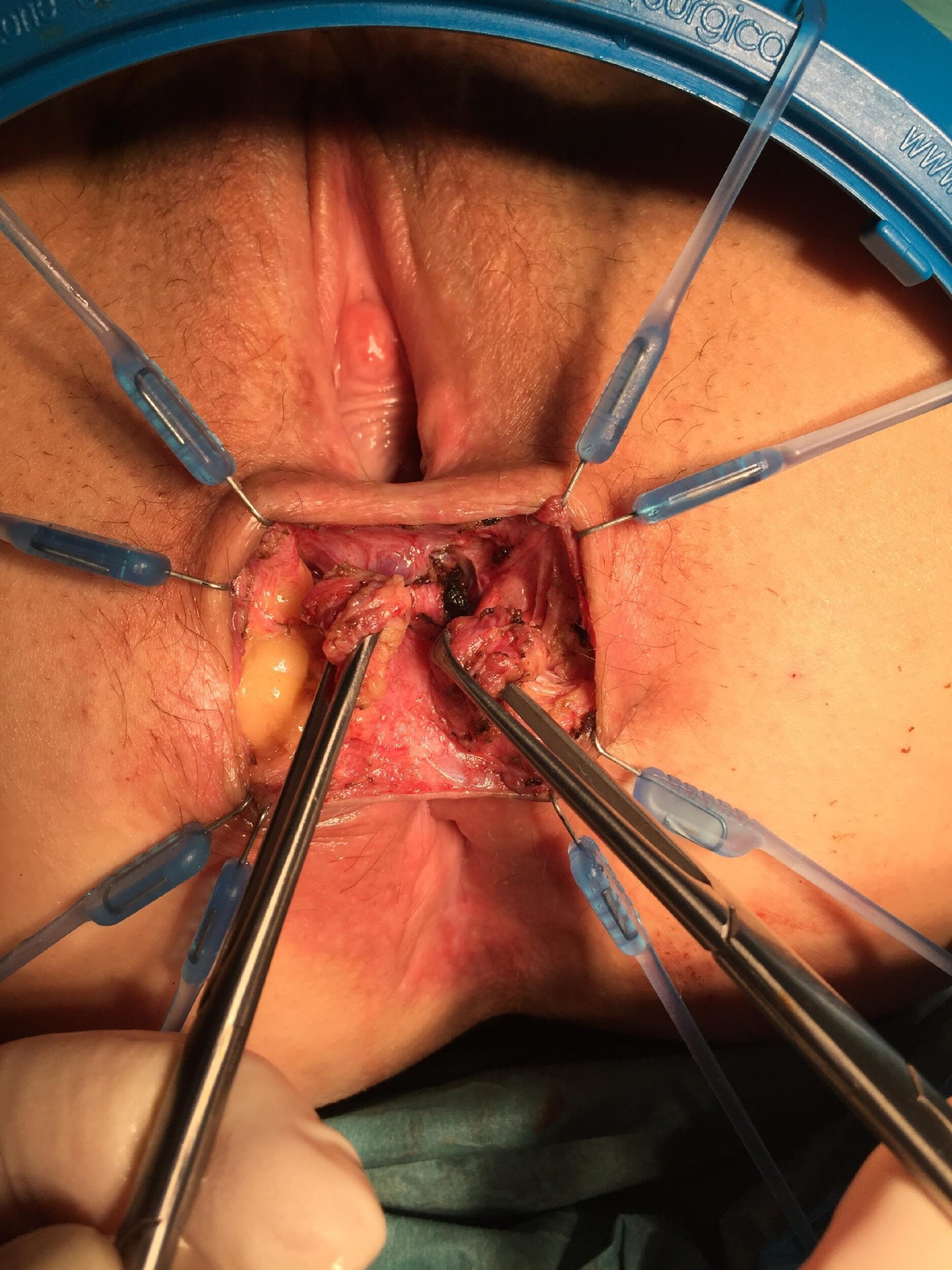
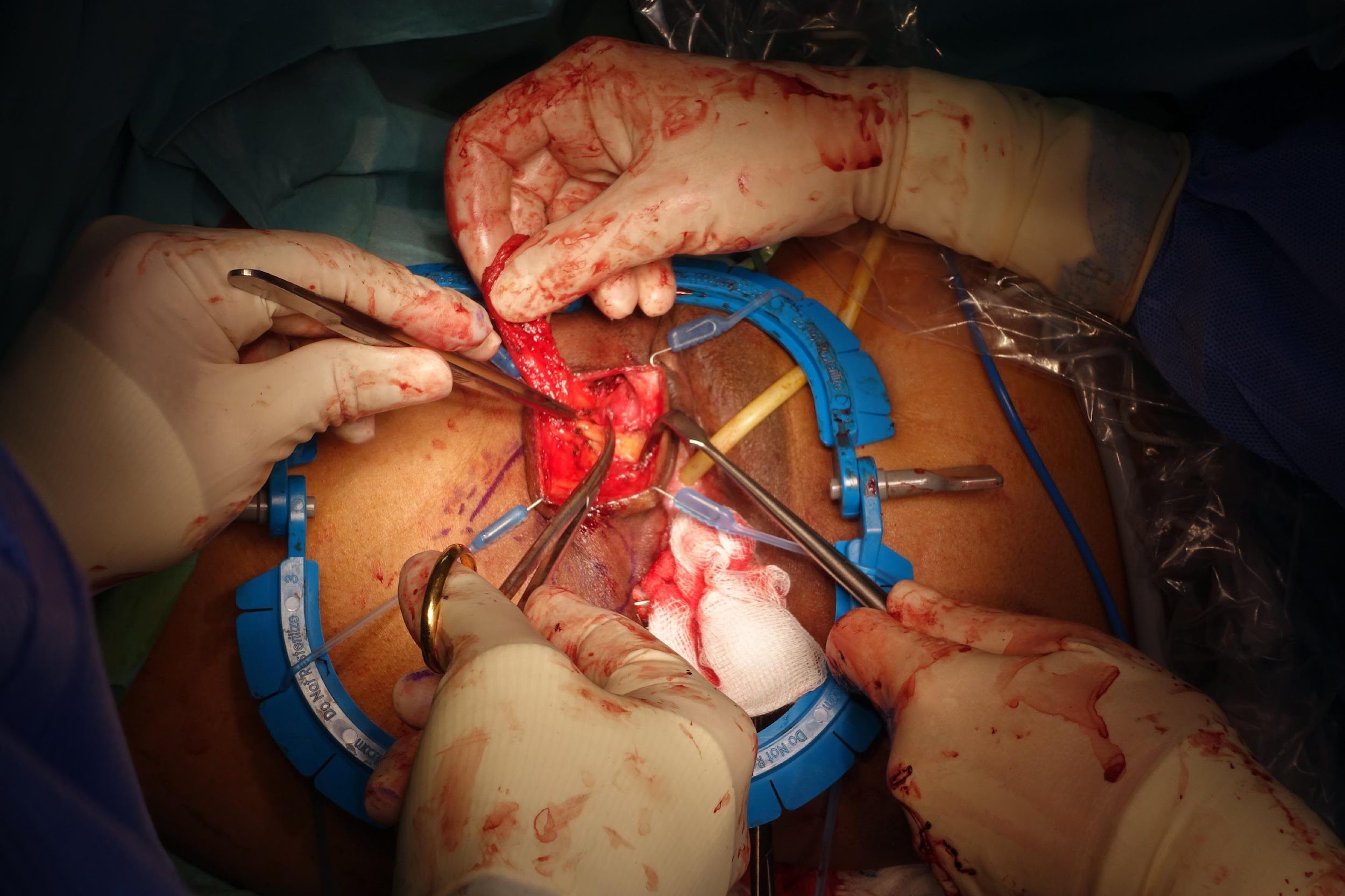
Sphinctero-plasty
these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing
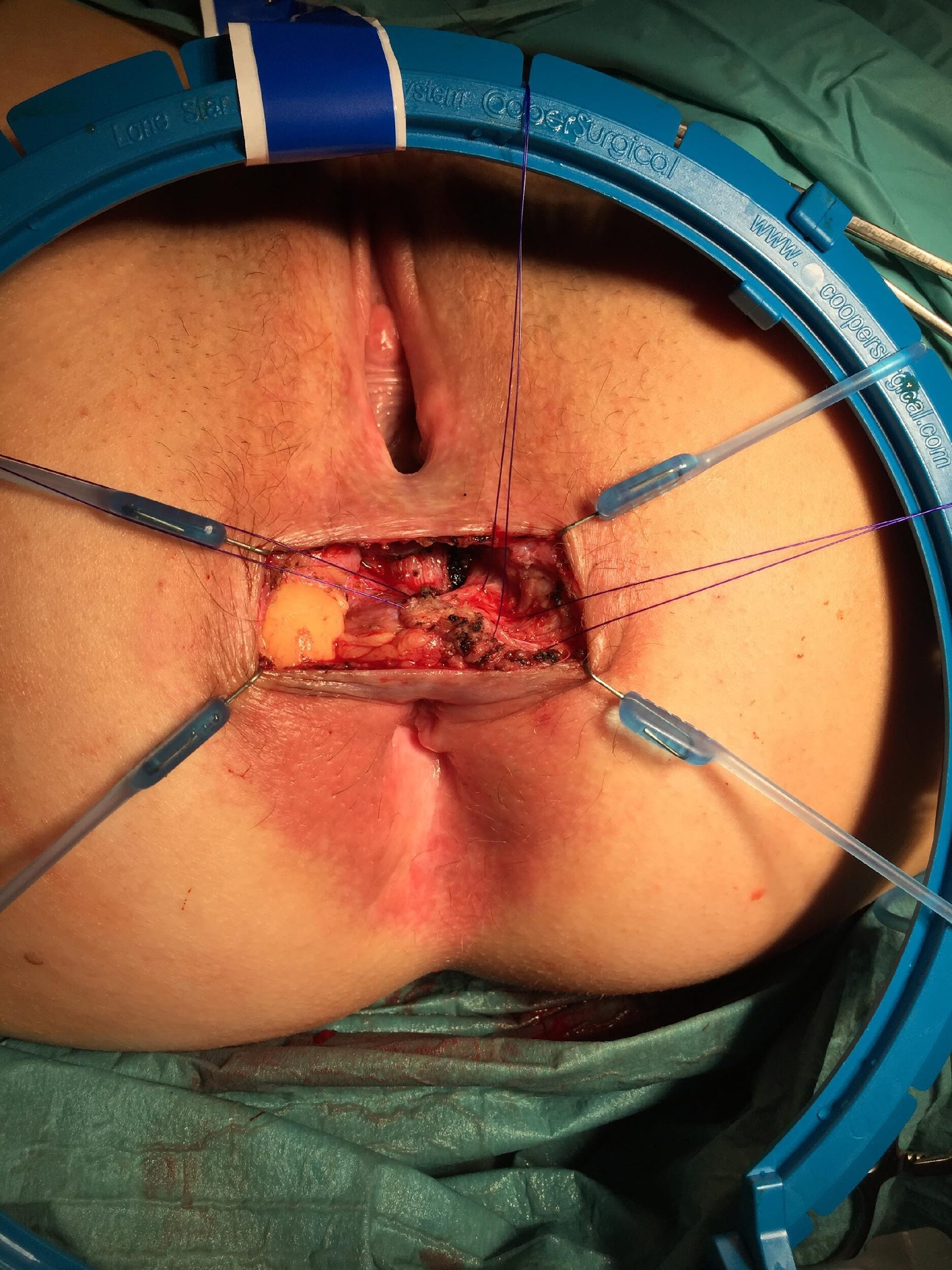
Sphinctero-plasty and Sphin-keeper together
these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing
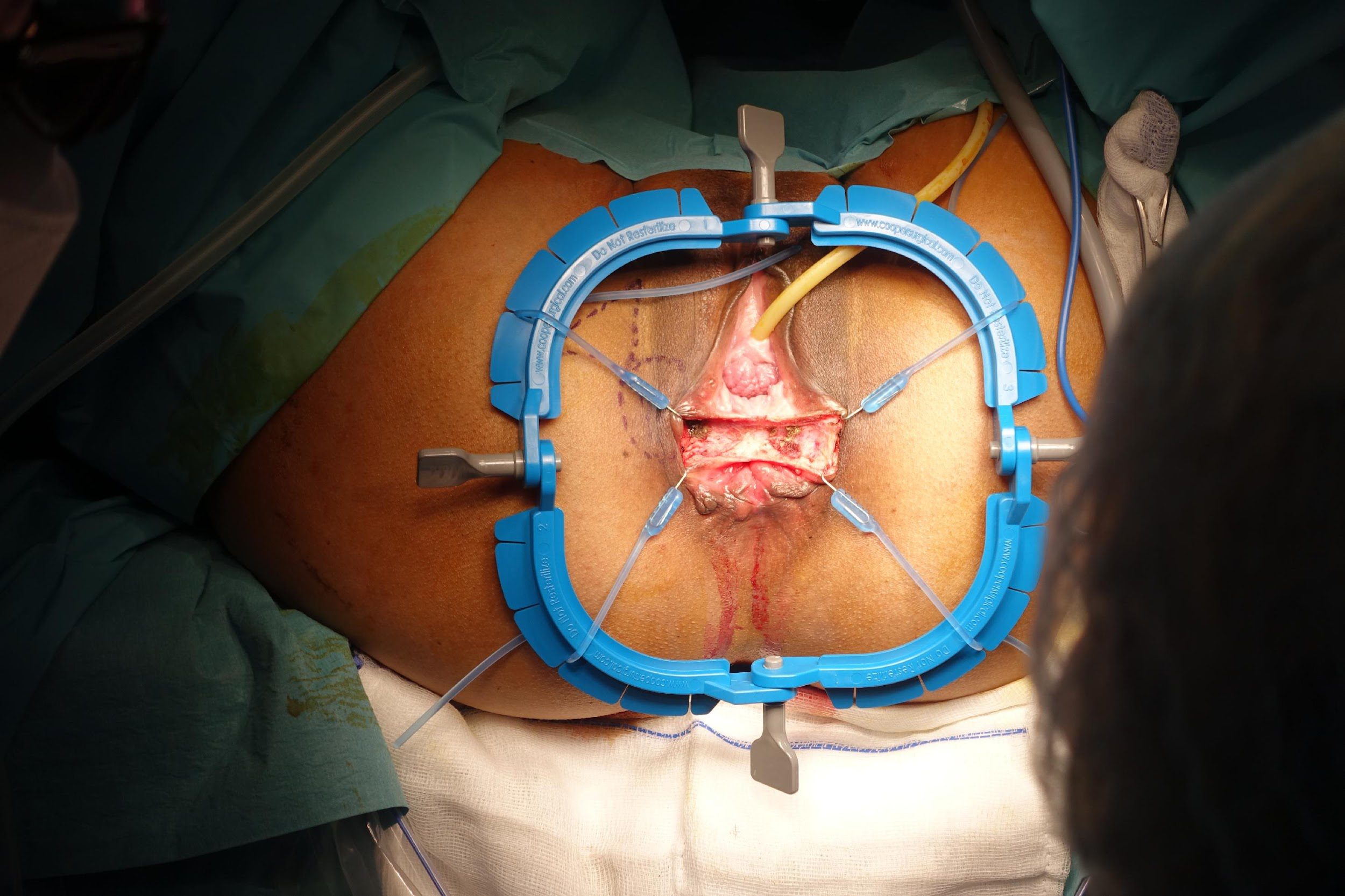
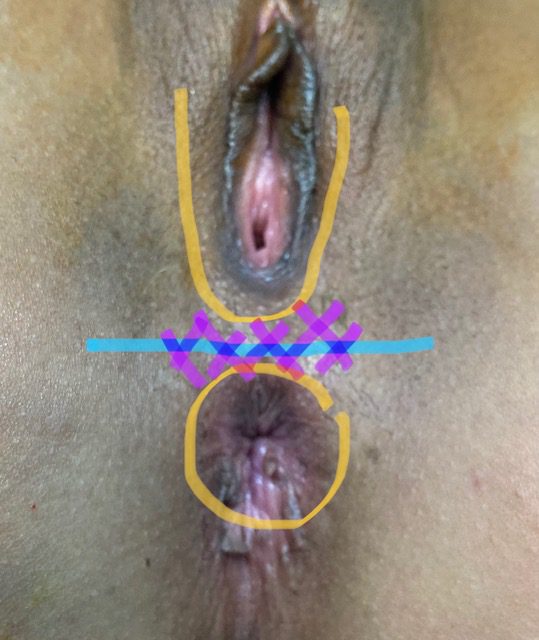
Repair of “Cloaca”
these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing
these photos contain sensitive content which some people may find offensive and disturbing
47.5 (35-64) years
16:1
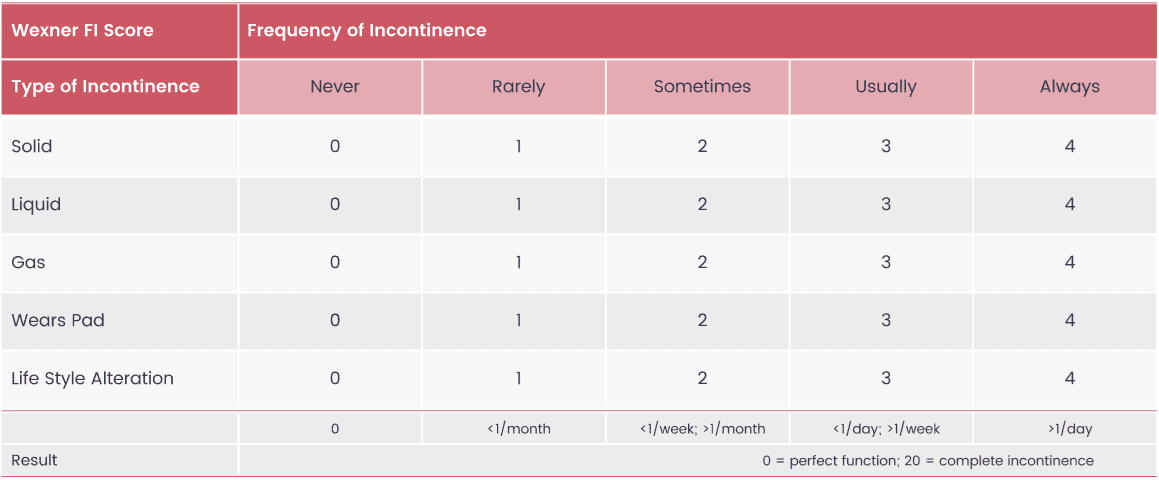
10.5/20 points
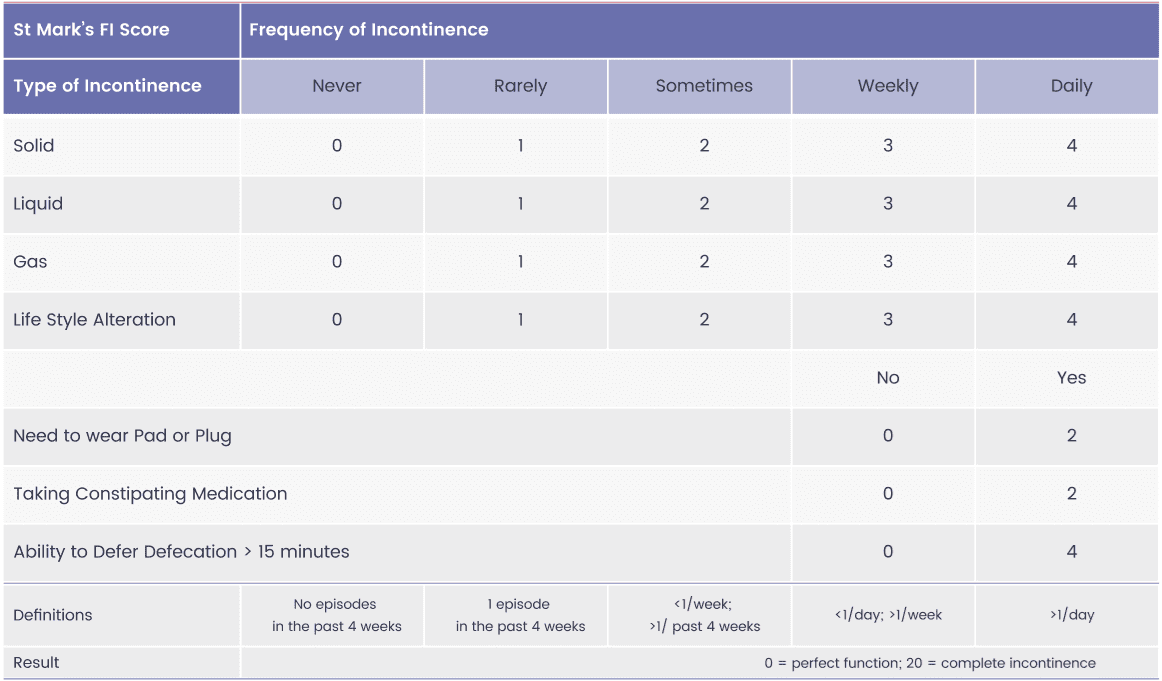
13.9/24 points
5.66/20 points
5.61/24 points
7.1 points



Mediclinic Dubai Mall The Dubai Mall, Fashion Parking, level 7 Book via 8001999
Mediclinic City Hospital
Dubai Health Care City, Building 37
Book via 8001999
Copyright © 2023